
| | |  Health & Beauty | November 2009 Health & Beauty | November 2009 
Surgery for Mental Ills Offers Both Hope and Risk
 Benedict Carey - New York Times Benedict Carey - New York Times
go to original
November 27, 2009
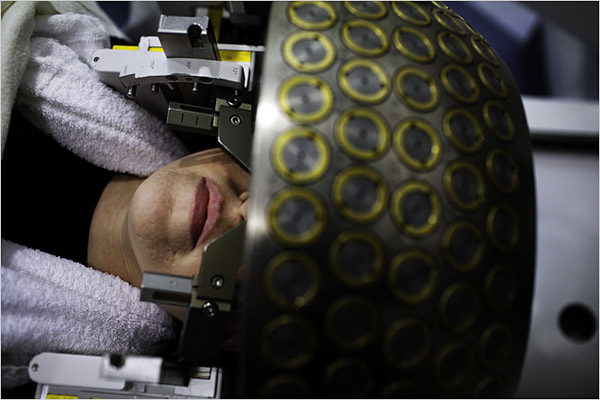
| | Karen Quintal, with a Leksell frame screwed into her skull before surgery for a tumor. (Christopher Capozziello/New York Times) | |
One was a middle-aged man who refused to get into the shower. The other was a teenager who was afraid to get out.
The man, Leonard, a writer living outside Chicago, found himself completely unable to wash himself or brush his teeth. The teenager, Ross, growing up in a suburb of New York, had become so terrified of germs that he would regularly shower for seven hours. Each received a diagnosis of severe obsessive-compulsive disorder, or O.C.D., and for years neither felt comfortable enough to leave the house.
But leave they eventually did, traveling in desperation to a hospital in Rhode Island for an experimental brain operation in which four raisin-sized holes were burned deep in their brains.
Today, two years after surgery, Ross is 21 and in college. “It saved my life,” he said. “I really believe that.”
The same cannot be said for Leonard, 67, who had surgery in 1995. “There was no change at all,” he said. “I still don’t leave the house.”
Both men asked that their last names not be used to protect their privacy.
The great promise of neuroscience at the end of the last century was that it would revolutionize the treatment of psychiatric problems. But the first real application of advanced brain science is not novel at all. It is a precise, sophisticated version of an old and controversial approach: psychosurgery, in which doctors operate directly on the brain.
In the last decade or so, more than 500 people have undergone brain surgery for problems like depression, anxiety, Tourette’s syndrome, even obesity, most as a part of medical studies. The results have been encouraging, and this year, for the first time since frontal lobotomy fell into disrepute in the 1950s, the Food and Drug Administration approved one of the surgical techniques for some cases of O.C.D.
While no more than a few thousand people are impaired enough to meet the strict criteria for the surgery right now, millions more suffering from an array of severe conditions, from depression to obesity, could seek such operations as the techniques become less experimental.
But with that hope comes risk. For all the progress that has been made, some psychiatrists and medical ethicists say, doctors still do not know much about the circuits they are tampering with, and the results are unpredictable: some people improve, others feel little or nothing, and an unlucky few actually get worse. In this country, at least one patient was left unable to feed or care for herself after botched surgery.
Moreover, demand for the operations is so high that it could tempt less experienced surgeons to offer them, without the oversight or support of research institutions.
And if the operations are oversold as a kind of all-purpose cure for emotional problems — which they are not, doctors say — then the great promise could quickly feel like a betrayal.
“We have this idea — it’s almost a fetish — that progress is its own justification, that if something is promising, then how can we not rush to relieve suffering?” said Paul Root Wolpe, a medical ethicist at Emory University.
It was not so long ago, he noted, that doctors considered the frontal lobotomy a major advance — only to learn that the operation left thousands of patients with irreversible brain damage. Many promising medical ideas have run aground, Dr. Wolpe added, “and that’s why we have to move very cautiously.”
Dr. Darin D. Dougherty, director of the division of neurotherapeutics at Massachusetts General Hospital and an associate professor of psychiatry at Harvard, put it more bluntly. Given the history of failed techniques, like frontal lobotomy, he said, “If this effort somehow goes wrong, it’ll shut down this approach for another hundred years.”
A Last Resort
Five percent to 15 percent of people given diagnoses of obsessive-compulsive disorder are beyond the reach of any standard treatment. Ross said he was 12 when he noticed that he took longer to wash his hands than most people. Soon he was changing into clean clothes several times a day. Eventually he would barely come out of his room, and when he did, he was careful about what he touched.
“It got so bad, I didn’t want any contact with people,” he said. “I couldn’t hug my own parents.”
Before turning to writing, Leonard was a healthy, successful businessman. Then he was struck, out of nowhere, with a fear of insects and spiders. He overcame the phobias, only to find himself with a strong aversion to bathing. He stopped washing and could not brush his teeth or shave.
“I just looked horrible,” he said. “I had a big, ugly beard. My skin turned black. I was afraid to be seen out in public. I looked like a street person. If you were a policeman, you would have arrested me.”
Both tried antidepressants like Prozac, as well as a variety of other medications. They spent many hours in standard psychotherapy for obsessive-compulsive disorder, gradually becoming exposed to dreaded situations — a moldy shower stall, for instance — and practicing cognitive and relaxation techniques to defuse their anxiety.
To no avail.
“It worked for a while for me, but never lasted,” Ross said. “I mean, I just thought my life was over.”
But there was one more option, their doctors told them, a last resort. At a handful of medical centers here and abroad, including Harvard, the University of Toronto and the Cleveland Clinic, doctors for years have performed a variety of experimental procedures, most for O.C.D. or depression, each guided by high-resolution imaging technology. The companies that make some of the devices have supported the research, and paid some of the doctors to consult on operations.
In one procedure, called a cingulotomy, doctors drill into the skull and thread wires into an area called the anterior cingulate. There they pinpoint and destroy pinches of tissue that lie along a circuit in each hemisphere that connects deeper, emotional centers of the brain to areas of the frontal cortex, where conscious planning is centered.
This circuit appears to be hyperactive in people with severe O.C.D., and imaging studies suggest that the surgery quiets that activity. In another operation, called a capsulotomy, surgeons go deeper, into an area called the internal capsule, and burn out spots in a circuit also thought to be overactive.
An altogether different approach is called deep brain stimulation, or D.B.S., in which surgeons sink wires into the brain but leave them in place. A pacemaker-like device sends a current to the electrodes, apparently interfering with circuits thought to be hyperactive in people with obsessive-compulsive disorder (and also those with severe depression). The current can be turned up, down or off, so deep brain stimulation is adjustable and, to some extent, reversible.
In yet another technique, doctors place the patient in an M.R.I.-like machine that sends beams of radiation into the skull. The beams pass through the brain without causing damage, except at the point where they converge. There they burn out spots of tissue from O.C.D.-related circuits, with similar effects as the other operations. This option, called gamma knife surgery, was the one Leonard and Ross settled on.
The institutions all have strict ethical screening to select candidates. The disorder must be severe and disabling, and all standard treatments exhausted. The informed-consent documents make clear that the operation is experimental and not guaranteed to succeed.
Nor is desperation by itself sufficient to qualify, said Richard Marsland, who oversees the screening process at Butler Hospital in Providence, R.I., which works with surgeons at Rhode Island Hospital, where Leonard and Ross had the operation.
“We get hundreds of requests a year and do only one or two,” Mr. Marsland said. “And some of the people we turn down are in bad shape. Still, we stick to the criteria.”
For those who have successfully recovered from surgery, this intensive screening seems excessive. “I know why it’s done, but this is an operation that could make the difference between life and death for so many people,” said Gerry Radano, whose book “Contaminated: My Journey Out of Obsessive-Compulsive Disorder” (Bar-le-Duc Books, 2007), recounts her own suffering and long recovery from surgery. She also has a Web site, freeofocd.com, where people from around the world consult with her.
But for the doctors running the programs, this screening is crucial. “If patients are poorly selected or not followed well, there’ll be an increasing number of bad outcomes, and the promise of this field will wither away,” said Dr. Ben Greenberg, the psychiatrist in charge of the program at Butler.
Dr. Greenberg said about 60 percent of patients who underwent either gamma knife surgery or deep brain stimulation showed significant improvement, and the rest showed little or no improvement. For this article, he agreed to put a reporter in touch with one — Leonard — who did not have a good experience.
The Danger of Optimism
The true measure of an operation, medical ethicists say, is its overall effect on a person’s life, not only on specific symptoms.
In the early days of psychosurgery, after World War II, doctors published scores of papers detailing how lobotomy relieved symptoms of mental distress. In 1949, the Portuguese neurologist Egas Moniz won the Nobel Prize in medicine for inventing the procedure.
But careful follow-up painted a darker picture: of people who lost motivation, who developed the helpless indifference dramatized by the post-op rebel McMurphy in Ken Kesey’s novel “One Flew Over the Cuckoo’s Nest,” played by Jack Nicholson in the 1975 movie.
The newer operations pinpoint targets on specific, precisely mapped circuits, whereas the frontal lobotomy amounted to a crude slash into the brain behind the eyes, blindly mangling whatever connections and circuits were in the way. Still, there remain large gaps in doctors’ understanding of the circuits they are operating on.
In a paper published last year, researchers at the Karolinska Institute in Sweden reported that half the people who had the most commonly offered operations for obsessive-compulsive disorder showed symptoms of apathy and poor self-control for years afterward, despite scoring lower on a measure of O.C.D. severity.
“An inherent problem in most research is that innovation is driven by groups that believe in their method, thus introducing bias that is almost impossible to avoid,” Dr. Christian Ruck, the lead author of the paper, wrote in an e-mail message. The institute’s doctors, who burned out significantly more tissue than other centers did, no longer perform the operations, partly, Dr. Ruck said, as a result of his findings.
In the United States, at least one patient has suffered disabling brain damage from an operation for O.C.D. The case led to a $7.5 million judgment in 2002 against the Ohio hospital that performed the procedure. (It is no longer offered there.)
Most outcomes, whether favorable or not, have had less remarkable immediate results. The brain can take months or even years to fully adjust after the operations. The revelations about the people treated at Karolinska “underscore the importance of face-to-face assessments of adverse symptoms,” Dr. Ruck and his co-authors concluded.
The Long Way Back
Ross said he felt no difference for months after surgery, until the day his brother asked him to play a video game in the basement, and down the stairs he went.
“I just felt like doing it,” he said. “I would never have gone down there before.”
He said the procedure seemed to give the psychotherapy sessions a chance to work, and last summer he felt comfortable enough to stop them. He now spends his days studying, going to class, playing the odd video game to relax. He has told friends about the operation, he said, “and they’re O.K. with it — they know the story.”
Leonard is still struggling, for reasons no one understands. He keeps odd hours, working through most nights and sleeping much of the day. He is not unhappy, he said, but he has the same aversion to washing and still lives like a hermit.
“I still don’t know why I’m like this, and I would still try anything that could help,” he said. “But at this point, obviously, I’m skeptical of the efficacy of surgery, at least for me.”
Ms. Radano, who wrote the book about her recovery, said the most important thing about the surgery was that it gave people a chance. “That’s all people in this situation want, and I know because I was there,” she said while getting into her car on a recent afternoon.
On the passenger seat was a container of decontaminating hand wipes. She pointed and laughed. “See? You’re never completely out.” |
|
| |

